American prescription drug pricing has always had a special talent for making simple things feel like advanced calculus. A medication can have a list price, a negotiated price, a coupon price, a pharmacy benefit manager price, a cash price, and a “please hold while your insurer thinks about it” price. So when the Trump administration launched TrumpRx, a new federal discount platform aimed at lowering what people pay for certain brand-name drugs, it instantly drew attention for one reason above all others: GLP-1s.
That makes sense. Drugs like Ozempic, Wegovy, and Zepbound have become the headliners of the modern prescription market. They are hugely popular, clinically important, and painfully expensive. For patients paying out of pocket, they can feel less like a monthly prescription and more like a second rent payment wearing a pharmacy label.
The big pitch behind TrumpRx is straightforward: give Americans one place to access lower prices on high-cost drugs, especially GLP-1 medications, without forcing them to wander through the internet like bargain hunters searching for socks and semaglutide in the same tab. The bigger question is whether the platform truly changes the economics of GLP-1 access or simply organizes discounts that were already creeping into the market.
The short answer? TrumpRx could make brand-name GLP-1s more affordable for some cash-paying patients, but it is not a magic wand, not a universal insurance fix, and definitely not the end of America’s long-running “why does this cost so much?” monologue.
What Is TrumpRx, Exactly?
TrumpRx is best understood as a federal drug discount portal, not a full replacement for health insurance and not a traditional government insurance benefit. The platform launched in early 2026 as part of the administration’s larger push to lower prescription drug prices and promote direct-to-consumer drug purchasing at reduced rates.
In plain English, TrumpRx is less “new insurance card in your wallet” and more “curated front door to lower cash prices.” For many drugs, the site either displays negotiated prices, points patients to manufacturer-run purchasing channels, or provides access to offers that reduce the gap between scary list prices and somewhat less scary real-world prices.
That distinction matters. A platform can absolutely lower costs for some people without changing the broader insurance system. But it also means patients still need to read the fine print, talk with their prescriber, and check whether they are paying cash, using insurance, or stepping into one of those murky zones where everyone assumes someone else explained the rules.
Why GLP-1s Became the Star of the Show
GLP-1 drugs are among the most in-demand prescription medications in the United States. These medicines mimic hormones involved in blood sugar control, appetite regulation, and satiety. Some are used for type 2 diabetes, some for obesity, and some now have additional indications tied to cardiovascular or sleep-related conditions.
Semaglutide products such as Ozempic and Wegovy, along with tirzepatide products such as Zepbound and Mounjaro, have driven a major shift in how patients, doctors, employers, and insurers think about chronic disease treatment. They are no longer niche specialty drugs. They are mainstream, high-demand therapies with broad medical and political visibility.
That popularity is exactly why pricing became such a flashpoint. These drugs can be transformative for the right patient, but they can also be brutally expensive when insurance excludes obesity treatment or applies strict prior authorization rules. Plenty of patients discover they are medically eligible long before they discover they are financially eligible. That is not great for morale.
How Much Could TrumpRx Lower GLP-1 Costs?
Headline prices that grabbed attention
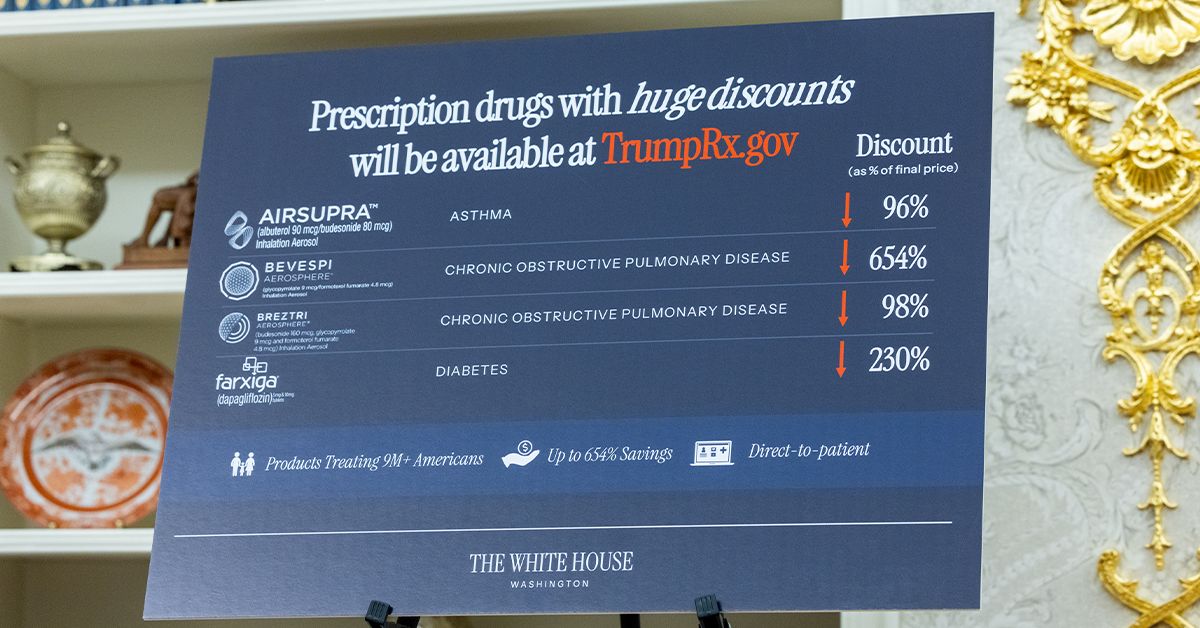
The administration promoted TrumpRx using steep discounts on GLP-1 medications as its flagship example. According to the White House’s published launch materials, monthly prices on the platform for Ozempic were described as falling from roughly $1,028 to an average of $350, while injectable Wegovy was described as dropping from roughly $1,349 to an average of $350 and as low as $199, depending on dose. The Wegovy pill was highlighted at as low as $149 per month, and Zepbound was promoted as falling from about $1,088 to an average of $346 and as low as $299.
Those numbers are significant because they change the conversation from “this is impossible” to “this is still expensive, but maybe not laugh-out-loud impossible.” For a patient who previously faced list-price shock, even a drop into the $199 to $350 range can mean the difference between filling the prescription and abandoning it at the pharmacy counter.
Why the numbers need context
Here is the part that deserves a yellow highlighter: those lower prices do not mean every patient pays the same amount. The actual cost can vary by dosage, product, eligibility terms, pharmacy channel, and whether the patient is using a manufacturer savings offer or a self-pay pathway. Some of the lowest advertised prices apply to starter doses, promotional periods, or narrow enrollment windows.
That is not unusual in the pharmaceutical world, but it does mean consumers should resist the urge to tattoo the lowest number onto their expectations. Drug pricing is a little like airline pricing. The advertised fare exists, but whether you personally get it depends on timing, route, terms, and how much patience you brought with you.
What TrumpRx Changes for Patients
The clearest benefit of TrumpRx is visibility. Before platforms like this, many patients had to piece together savings information from manufacturer websites, pharmacy tools, telehealth platforms, coupon sites, and insurer portals that all seemed designed by different planets. TrumpRx creates a centralized path for comparing lower cash prices on certain drugs and connecting patients with participating channels.
That matters most for people in a frustrating middle category: patients who have a valid prescription, want a brand-name GLP-1, and either do not have insurance coverage for obesity treatment or do not want to wait through multiple rounds of prior authorization, appeals, and existential sighing.
For those patients, TrumpRx can function like a shortcut. It does not make the drugs cheap in an absolute sense, but it may make them meaningfully less expensive and easier to access than the old list-price model ever did.
What TrumpRx Does Not Fix
Now for the less glamorous truth. TrumpRx does not solve every barrier tied to GLP-1 access.
First, it is largely designed for cash-paying consumers. That means purchases often occur outside the normal insurance benefit. In practical terms, patients may save money up front but may also find that the purchase does not count toward their deductible. A lower pharmacy bill is nice. Discovering it did not help your broader health plan math is less nice.
Second, it does not guarantee coverage for obesity treatment under employer plans, individual plans, Medicare, or Medicaid. Coverage rules remain a patchwork. Some patients will still run into utilization controls, denied claims, step therapy, or the classic American healthcare riddle: “Your doctor says yes, your insurer says maybe, and your budget says absolutely not.”
Third, it does not erase the fact that even discounted GLP-1s are still expensive for many households. A $299 or $349 monthly medication can be a good deal relative to a $1,300 list price while still being unaffordable in real life. Two things can be true at once. America is talented at that.
Why Prices Were Already Moving Before TrumpRx
One reason the TrumpRx rollout sparked debate is that GLP-1 prices were already under pressure before the platform launched. Drugmakers had been expanding direct-purchase options, adjusting self-pay offers, and responding to competition from telehealth firms and compounded products. In other words, TrumpRx entered a market that was already changing fast.
Novo Nordisk had already been promoting lower cash pricing on Wegovy through its own pharmacy and savings infrastructure. Eli Lilly had already built out LillyDirect and self-pay options for Zepbound. By the time TrumpRx arrived, the market for GLP-1s was no longer just about insurance reimbursement. It had become a cash-pay battlefield.
That does not mean TrumpRx is meaningless. It means the platform may be acting as an accelerator and organizer rather than the sole cause of lower prices. The White House gave the trend a political banner and a central website. The underlying price movement, however, was also being driven by market competition, manufacturer strategy, and consumer demand.
The Safety Question: Lower Prices Should Not Mean Lower Standards
No discussion of affordable GLP-1s is complete without talking about compounded versions. During shortages and the rapid boom in demand, compounded GLP-1 products spread quickly through telehealth channels and alternative suppliers. Many patients were drawn in by one obvious fact: they were often cheaper.
But the FDA has repeatedly warned that compounded GLP-1 drugs are not FDA-approved. The agency has raised concerns about improper storage, shipping quality, misleading marketing, and claims that suggest compounded products are identical to branded medicines when they are not. It has also warned dozens of telehealth companies over illegal marketing practices tied to compounded GLP-1s.
That is a major reason the TrumpRx conversation matters. If patients can buy authentic branded GLP-1 medications at lower cash prices, some may move away from riskier alternatives. For people who were choosing between a too-expensive approved drug and a cheaper gray-area version, the emergence of lower official prices could make that decision a lot less messy.
How Medicare and Medicaid Fit Into the Bigger Picture
TrumpRx is only one piece of the broader GLP-1 affordability story. Another big development is the administration’s separate work through CMS, including the BALANCE model, which is meant to expand access to GLP-1 drugs under Medicare and Medicaid pathways.
CMS has said a new GLP-1 payment demonstration is scheduled to begin in July 2026 as a bridge to the BALANCE model, with eligible Medicare beneficiaries paying $50 per month for covered GLP-1 medications. That is a very different lane from the TrumpRx cash-pay portal, but together the two efforts show a broader strategy: lower the price for cash buyers now while building separate public-program access pathways over time.
Even so, public coverage remains uneven. Medicaid coverage of GLP-1s for obesity is still limited across states, and many plans continue to worry about the long-term budget impact. That concern is not imaginary. Analysts have warned that broad GLP-1 coverage could create major spending pressures for Medicare and other payers, even if long-term health benefits are substantial.
Who Benefits Most From TrumpRx?
The patients most likely to benefit are those who fall into one of three groups.
1. Cash-paying patients with no obesity-drug coverage
This is the obvious group. If your health plan refuses to cover Wegovy or Zepbound for weight loss, a lower cash price can be genuinely valuable.
2. Patients who want authentic brand-name GLP-1s outside insurer delays
Some people would rather pay a lower published price than spend months fighting an insurer. Not ideal, but very American.
3. Patients comparing brand-name options against compounded alternatives
If TrumpRx makes approved drugs more reachable, it could pull some consumers toward products with clearer quality controls and established safety oversight.
The people who may still feel stuck include patients on fixed incomes, households facing long-term chronic use costs, and anyone who assumed “discounted” would mean “cheap enough to stop thinking about it.” For many families, it will not.
So, Is TrumpRx a Breakthrough or a Branded Coupon Book?
Honestly, it is a little of both.
TrumpRx is a real shift in how the federal government is presenting and channeling lower drug prices, especially for GLP-1s. It creates a more visible consumer marketplace for discounts and gives the administration a concrete answer to one of the country’s loudest health-cost complaints.
At the same time, the platform does not erase the deeper structural problems in prescription drug pricing. Insurance still behaves like insurance. Coverage still varies. Deductibles still exist. Manufacturer pricing still involves strategy, competition, and selective discounts. And “affordable” remains a highly personal word when you are staring at a monthly payment that could also buy groceries, utilities, or a very nice used lawn mower.
The real significance of TrumpRx may be that it acknowledges something the market has been screaming for years: patients want transparent, direct, lower-cost access to GLP-1s. Whether the platform becomes a lasting fix or just the first draft of a new model will depend on participation, pricing durability, public awareness, and how successfully it integrates with the rest of the healthcare system.
The Real-World Experience: What This Could Feel Like for Patients, Doctors, and Families
To understand TrumpRx, it helps to move beyond policy language and think about the everyday experience around these drugs.
Imagine a patient with obesity whose employer plan does not cover weight-loss medications. Before TrumpRx, she might leave her doctor’s office excited, hit the pharmacy counter, hear the price, and instantly begin a new hobby called “staring into the middle distance.” With a lower cash option, the conversation changes. The drug may still be expensive, but it is now within the realm of possible budgeting. That is not nothing. It can mean the difference between starting treatment and shelving the idea for another year.
Now picture a primary care doctor. For the past two years, that doctor has probably spent too much time discussing coverage denials, shortages, coupon programs, and whether a patient’s online source is selling a legitimate product or a chemistry experiment with branding. A platform that offers more straightforward access to approved GLP-1s can make those conversations easier. Doctors still need to counsel patients on side effects, expectations, dose escalation, and long-term treatment plans, but fewer detours into pricing chaos is a win.
Pharmacists may also feel the change. They are often the people left explaining why a drug that was medically recommended is financially absurd. When published cash prices are lower and easier to find, pharmacists can help patients compare legitimate options with fewer rounds of confusion. In a retail setting, that matters because every minute spent untangling insurance drama is a minute not spent on medication safety, adherence counseling, or the 47 other things pharmacists quietly save the healthcare system from every day.
Families, meanwhile, may experience TrumpRx as a budgeting tool rather than a policy event. One spouse might say, “It used to be over a thousand dollars, now it’s three hundred.” The other spouse might reply, “Three hundred is still a lot.” Both are correct. The practical experience of GLP-1 treatment is not just clinical. It is financial, emotional, and often tied to long-term goals around blood sugar control, heart health, weight management, and quality of life.
There is also a trust issue. Many consumers have grown skeptical after years of flashy promises in healthcare. So even when prices do come down, some people will wonder whether the savings are temporary, dose-specific, or loaded with exclusions. That caution is reasonable. Patients have learned to read the asterisk because the asterisk has hurt them before.
In that sense, the lived experience of TrumpRx may be less about political branding and more about whether ordinary people feel one simple thing: relief. If a patient can get an authentic GLP-1 more easily, more safely, and at a price that no longer feels like a financial jump scare, the program will feel real. If not, it risks becoming another glossy healthcare promise that looked great on launch day and less impressive at the kitchen table.
Conclusion
TrumpRx could lower the cost of GLP-1s for many cash-paying Americans, especially those shut out by spotty insurance coverage for obesity treatment. That is the good news, and it is real. Lower visible prices for Ozempic, Wegovy, and Zepbound could pull patients toward approved medicines and away from riskier alternatives.
But the program is not a full rewrite of prescription drug access in America. It is a discount platform, not a universal entitlement. It can reduce the sticker shock without eliminating the broader affordability problem. For patients, the smartest approach is still the boring one: compare channels, confirm eligibility, ask whether the drug is FDA-approved, and talk through long-term costs with a prescriber before assuming the “low” price will stay low forever.
In other words, TrumpRx may be a meaningful step in the GLP-1 price war, but it is not the final boss. Not even close.